
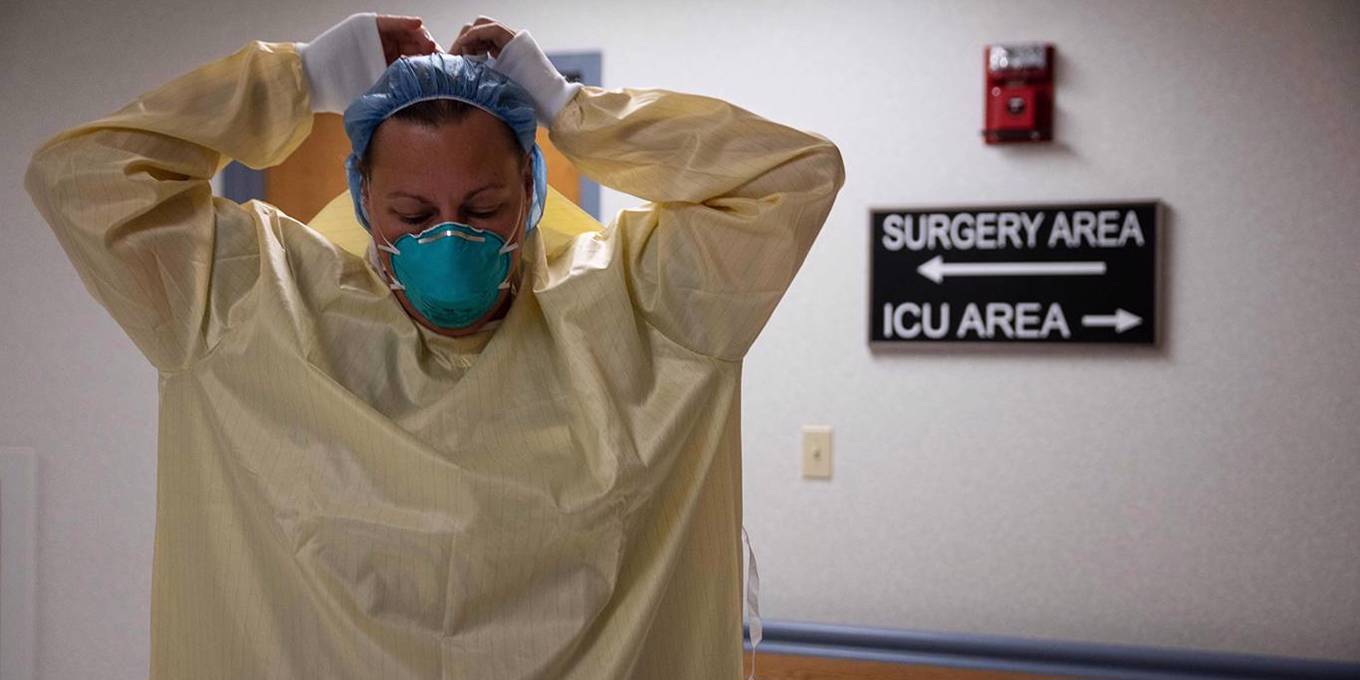
America desperately needs a supply-side revolution to unclog the arteries of its health care system and offset an increasingly urgent shortage of doctors. As things stand, new medical schools, qualified doctors, and well-tested drugs all face unnecessary hurdles.
SAN DIEGO — Between 1980 and 2000, the U.S. National Basketball Association added six teams, while the National Football League and Major League Baseball added four each. How many medical schools has the United States added? None. In many cities, it may now be easier to find a light-footed quarterback than a pediatrician.
For years the American Medical Association has stopped the flow of new students, affirming in 1997 that “the United States is on the brink of a serious shortage of doctors”. Now we see the results: Overworked nurses in Minneapolis are walk on the picket lines demanding 30% wage increases; and rural hospitals and health care providers across the country are chronically short of doctors.
The situation calls for a supply revolution to unclog the arteries of the health system. We have already seen what a surge in supply can do in other sectors. In the hotel industry, the arrival of Airbnb indeed added 25% more hotel rooms nationwide, making it harder for hotels to raise prices.
Why haven’t we seen similar developments in healthcare? In fact, we have, but only in areas free from entrenched interest groups and government over-regulation. For example, there is healthy competition to provide elective procedures like LASIK eye surgery and Botox. In the decade since LASIK was approved in 1999, thousands of surgeons have learned to target corneas with lasers, bringing the price down in 25%. Botox, meanwhile, has to compete with Dysport and Jeuveau, while dermatologists compete with cosmetologists in spas. This market dynamic provides better prices for frowning consumers across the country.
Unfortunately, the same cannot be said for the sectors that are more important to people’s basic health. By 2026, the proportion of U.S. physicians reaching retirement age jump from 12% to 21%. Many will choose golf or mahjong over maintaining a medical practice or being on call in a hospital. And even though universities have finally opened more medical schools, the number of new graduates cannot keep up with the growing demands of an aging population. As a result, the Association of American Medical Colleges (AAMC) predicts a shortage of up to 124,000 doctors by 2034.
And the United States is not alone. One in five people in Ireland is expect see a doctor, and in Canada a Chihuahua can get a computed tomography for cancer more easily than a human being.
Subscribe to PS Digital
Access to all news PS commentary, our entire On Point suite of subscriber-exclusive content – including longer reads, insider interviews, Big Picture/Big Question and Say More – and the full PS archive.
A supply-side health care revolution would break down the barriers that impede the supply of qualified physicians and proven medicines. As it stands, it may take $200 million and ten years before the Liaison Committee on Medical Education (reporting to the U.S. Department of Education) investigates, schedules hearings, and ultimately grants approval for a new medical school. And that’s just the beginning. Even if a faculty of medicine opens, graduates struggle to find residency places to complete their training, because a law of 1997 froze the number of residences by tying them to Medicare spending. Congress should lift that cap.
In addition, medical training should be streamlined. In 2015, the AAMC revised the Medical College Admission Test to encourage students to devote more time to empathy and sociology. Applicants are now asked to define terms such as “social constructionism.” But while empathy is important, it won’t help patients who are on the waitlist for procedures or who reside in areas where there are no doctors.
To increase supply, the United States should follow other developed countries in allowing aspiring doctors to begin their medical training as undergraduate students. At the University of Cambridge, medical students examine their first corpses at 18, rather than waiting until 22. In the United States, a typical medical school graduate initially spends four years taking undergraduate courses and racking up crippling debt.
The United States should also ease the way for foreign doctors who have already undergone rigorous testing in other advanced economies. Let’s say you are a cardiologist practicing for 20 years in Germany or Singapore. Even if the US immigration authorities let you into the country, you will still have to go through a series of increasingly tight hoopsincluding federal and state licensing exams, clinical skills labs, and an all-new multi-year residency at a US hospital.
Likewise, the Food and Drug Administration should make the way easier for drugs that have been tested, approved and deployed in other developed countries. Typically, the FDA requires pharmaceutical companies to spend tens of millions of dollars and many years repeating successful clinical trials, as if Americans (albeit beefier ones) were a different species from the humans we find elsewhere.
Consider what the current system has done. In 2013, a deadly strain of meningitis spread through dormitories at Princeton University, forcing school administrators to beg the government to allow them access to a Swiss vaccine manufactured by Novartis. When monkeypox hit the United States and Europe this summer, European regulators were quick to approved an effective antiviral against smallpox, but the Americans had to wait, even though the United States had a stockpile of 1.7 million doses. The FDA delayed because it wanted the National Institutes of Health to conduct a multi-year randomized control experiment, as if the epidemic was waiting.
Epidemics don’t wait, of course – and neither do we. While we can’t predict the next wave of meningitis or monkeypox, we can certainly avoid a man-made epidemic of untreated patients searching in vain for someone who can help them.
Comments are closed.